
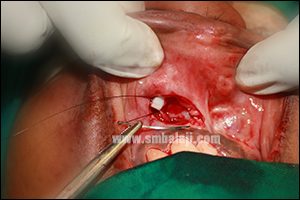
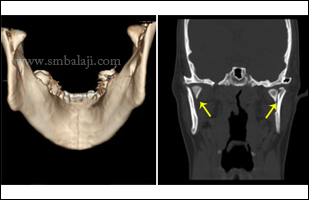
A 35-year-old female reported to our hospital with a complaint of severe pain and swelling with respect to her upper front teeth. A digital x-ray revealed a large cystic lesion at the root apex of maxillary right central and lateral incisor with resorption of the roots.
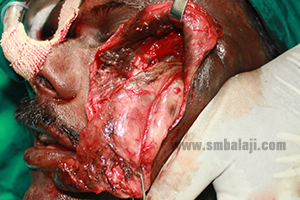
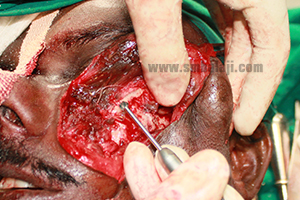
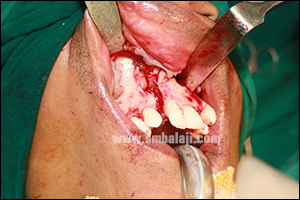
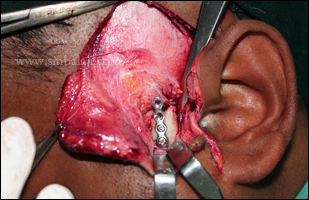
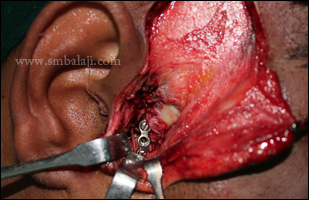
Maxillofacial Surgeon Dr. S.M. Balaji accessed the cystic lesion raising a gingivomucoperiosteal flap and completely enucleated the cyst. The affected teeth were extracted. The removal of the lesion left a large bone defect. For complete closure of the defect and to enable implant placement in future, the defect size was measured, a bone graft of the same size was harvested from the mandibular symphysis and placed in the bone defect successfully closing it. After subsequent healing, implants & ceramic crowns will be placed for fixed replacement of lost teeth.
Maxillofacial Surgeon Dr. S.M. Balaji accessed the cystic lesion raising a gingivomucoperiosteal flap and completely enucleated the cyst. The affected teeth were extracted. The removal of the lesion left a large bone defect. For complete closure of the defect and to enable implant placement in future, the defect size was measured, a bone graft of the same size was harvested from the mandibular symphysis and placed in the bone defect successfully closing it. After subsequent healing, implants & ceramic crowns will be placed for fixed replacement of lost teeth.






































































 RSS Feed
RSS Feed