
Surgical correction of nose deformities also known as the “Nose Job” requires expertise and experience. The surgeons estimate the type of defect - either excess or deficit of the height, deviations, depressions and abnormally angled noses. The patient’s expectation of his/her nose is understood after careful examination.
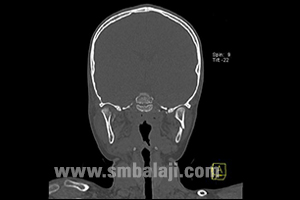
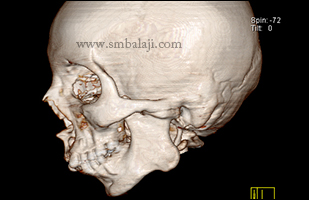
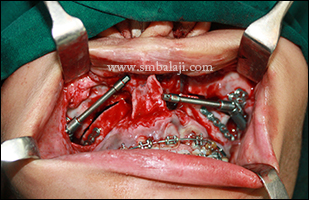
Shown is a case with a deficiency of the bridge portion of nose. Note the midlevel of the nasal bone, where there is a deficiency creating a huge impact on the patient’s facial profile. This gives the nose a saddle-shape. Tip of the nose appears bulky and everted in the profile view; base of the nose appears broad. Maxillofacial Surgeon Dr. S.M. Balaji planned a closed rhinoplasty technique wherein the surgical approach is through the nose to prevent unsightly scars.
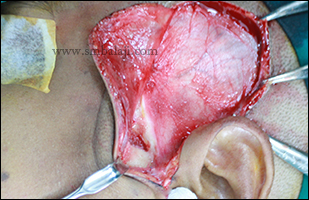
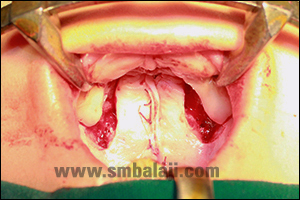
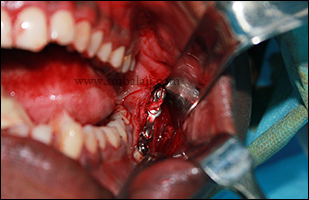
Appropriate measurement of nose was made and the amount of augmentation needed was noted. Autologous graft (rib graft) was harvested, shaped and positioned to improve the aesthetics of the nose. Bulky nose tip was corrected by removing the prominent lower lateral nasal septal cartilage and Weir excision done to reduce the width of the alar base. Results are immediate. The patient is very happy with the surgery outcome and his enhanced appearance without any visible surgical marks
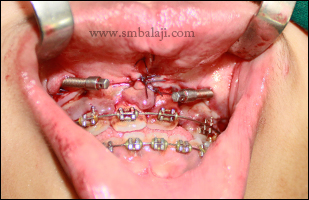
Shown is a case with a deficiency of the bridge portion of nose. Note the midlevel of the nasal bone, where there is a deficiency creating a huge impact on the patient’s facial profile. This gives the nose a saddle-shape. Tip of the nose appears bulky and everted in the profile view; base of the nose appears broad. Maxillofacial Surgeon Dr. S.M. Balaji planned a closed rhinoplasty technique wherein the surgical approach is through the nose to prevent unsightly scars.
Appropriate measurement of nose was made and the amount of augmentation needed was noted. Autologous graft (rib graft) was harvested, shaped and positioned to improve the aesthetics of the nose. Bulky nose tip was corrected by removing the prominent lower lateral nasal septal cartilage and Weir excision done to reduce the width of the alar base. Results are immediate. The patient is very happy with the surgery outcome and his enhanced appearance without any visible surgical marks







































 RSS Feed
RSS Feed