
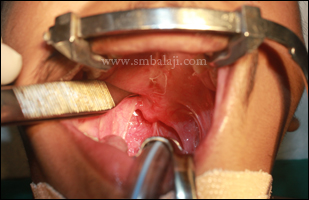
A 15 year old boy with unilateral cleft lip and palate reported to our hospital with the complaints of slurred speech. Cleft lip, palate correction and bone grating were done in their hometown during his childhood. He gave the history of flap pharyngoplasty done elsewhere 1 year back.
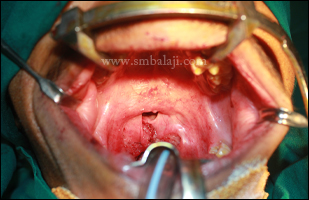
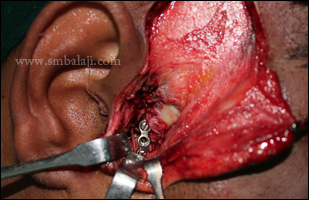
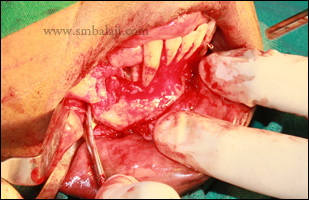
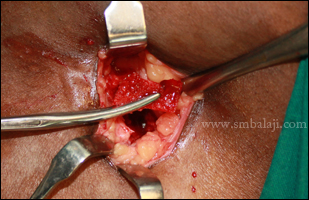
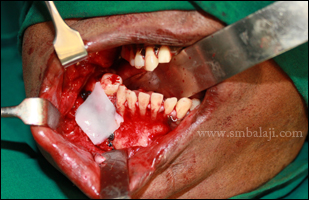
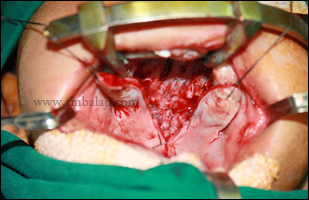
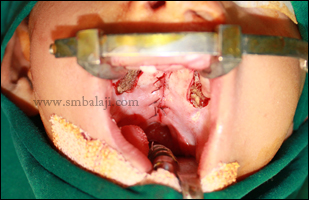
Maxillofacial surgeon Dr. S. M. Balaji skillfully diagnosed and concluded that his defective speech was due to Velopharyngeal incompetence by abnormal suturing of soft palate muscle. Thus he expertly planned to correct his speech by re positioning the pharyngeal muscles in such a way, soft palate movement will be enhanced and dynamic sphincter will be created. Thus re pharyngoplasty was performed successfully and suction test was done after the procedure which indicates positive results due to excellent soft palate movement enhancing the sphincter muscle activity. Immediate results were shown in the following video.
Maxillofacial surgeon Dr. S. M. Balaji skillfully diagnosed and concluded that his defective speech was due to Velopharyngeal incompetence by abnormal suturing of soft palate muscle. Thus he expertly planned to correct his speech by re positioning the pharyngeal muscles in such a way, soft palate movement will be enhanced and dynamic sphincter will be created. Thus re pharyngoplasty was performed successfully and suction test was done after the procedure which indicates positive results due to excellent soft palate movement enhancing the sphincter muscle activity. Immediate results were shown in the following video.
VIDEO: Intra oral video after surgery showing suction test positive thus dynamic sphincter created












































































































 RSS Feed
RSS Feed