
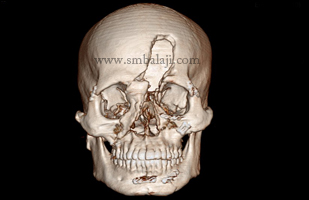
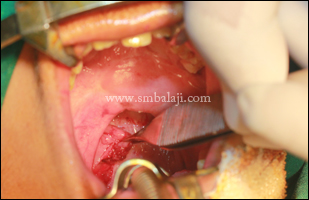
A 10-year-old boy was brought to our hospital by his parents for reconstruction of his alveolar cleft. He was previously operated for cleft lip and cleft palate in his childhood. On his parents’ request he was planned to undergo bone graft surgery.
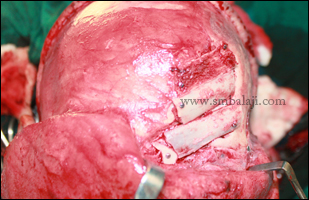
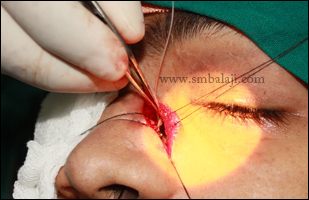
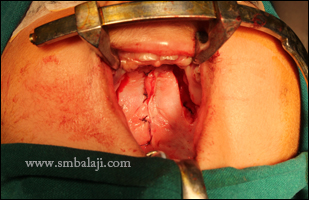
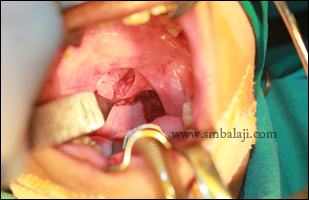
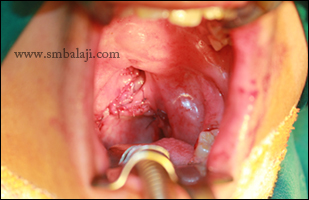
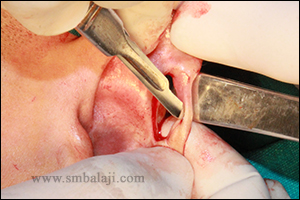
Maxillofacial Surgeon Dr. S.M. Balaji grafted bone from the boy’s hip region and the harvested bone was jam packed in the cleft to completely close the defect. Closure of alveolar cleft defect either by bone graft or BMP will ensure proper eruption of permanent teeth. Further cleft management will be done subsequently.
Maxillofacial Surgeon Dr. S.M. Balaji grafted bone from the boy’s hip region and the harvested bone was jam packed in the cleft to completely close the defect. Closure of alveolar cleft defect either by bone graft or BMP will ensure proper eruption of permanent teeth. Further cleft management will be done subsequently.




























































































 RSS Feed
RSS Feed