







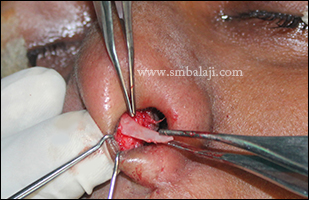
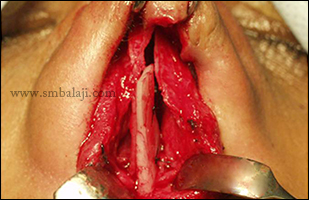
A young man had met with a motor vehicular accident a few days in which he had sustained injuries to his lower jaw. He had severe jaw pain, his teeth occlusion was completely deranged and he had great difficulty in biting, chewing, swallowing and speaking.
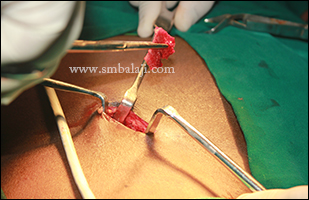
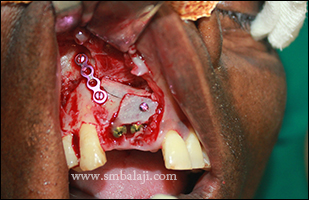
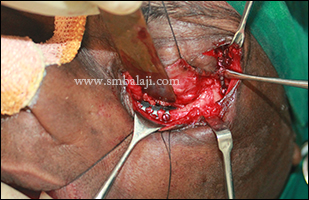
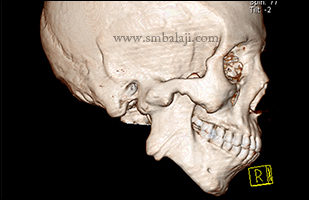
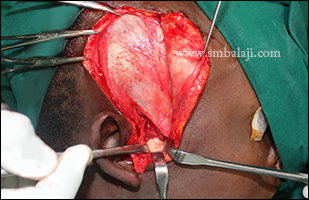
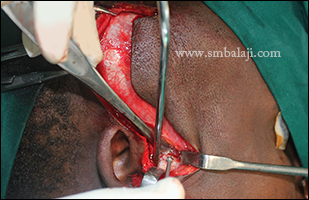
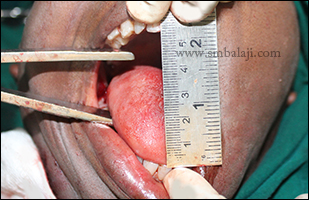
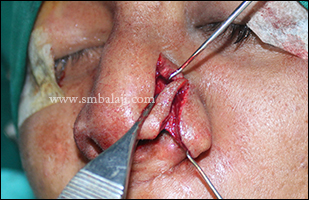
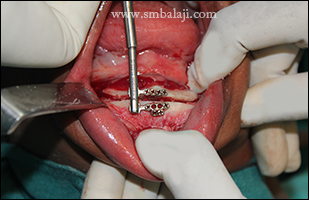
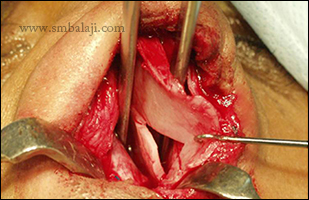
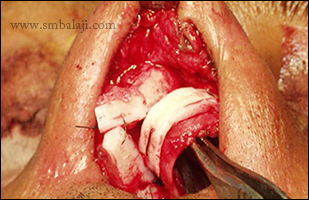
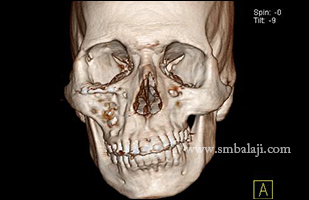
A preoperative 3D CT scan revealed fracture in the right mandibular parasymphysis region and left angle of mandible. Maxillofacial Surgeon Dr. S.M. Balaji successfully fixed and stabilized the fractured segments using bone plates and screws. The fractured tooth in the line of fracture was extracted. Accurate occlusion and bite was achieved. Postsurgery radiograph showed optimum fracture fixation.
A preoperative 3D CT scan revealed fracture in the right mandibular parasymphysis region and left angle of mandible. Maxillofacial Surgeon Dr. S.M. Balaji successfully fixed and stabilized the fractured segments using bone plates and screws. The fractured tooth in the line of fracture was extracted. Accurate occlusion and bite was achieved. Postsurgery radiograph showed optimum fracture fixation.


























































 RSS Feed
RSS Feed