
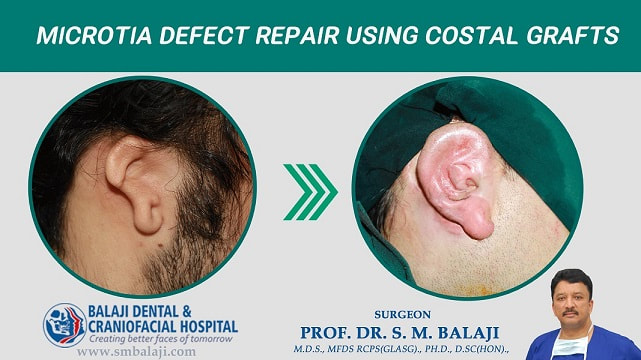
Microtia Defect Repair using Costal Grafts
This gentleman was born with microtia of the right ear. Microtia is the congenital deformity of the external ear. Reconstructive surgery is performed in two stages. He presented to our hospital for surgical correction of his microtia ear deformity.
A template was first made using the left ear to ensure that the reconstructed right ear was symmetrical to the normal left ear. Costal rib graft with perichondrium was then harvested from the patient. The graft was crafted using the template for reconstruction of the right ear. Markings were made in the region of the deformed right ear and a subcutaneous pocket was created. The crafted cartilaginous graft was placed in the pocket and the incision was closed with sutures.
The second stage was performed in four months with lifting up of the cartilaginous graft along with placement of a skin graft in the postauricular region. This resulted in reconstruction of a symmetrical right external ear.
A template was first made using the left ear to ensure that the reconstructed right ear was symmetrical to the normal left ear. Costal rib graft with perichondrium was then harvested from the patient. The graft was crafted using the template for reconstruction of the right ear. Markings were made in the region of the deformed right ear and a subcutaneous pocket was created. The crafted cartilaginous graft was placed in the pocket and the incision was closed with sutures.
The second stage was performed in four months with lifting up of the cartilaginous graft along with placement of a skin graft in the postauricular region. This resulted in reconstruction of a symmetrical right external ear.










































 RSS Feed
RSS Feed