
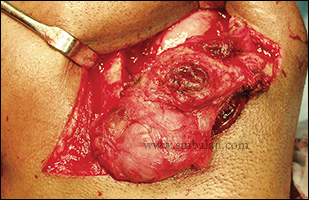
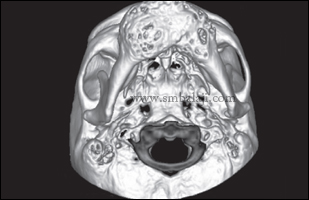
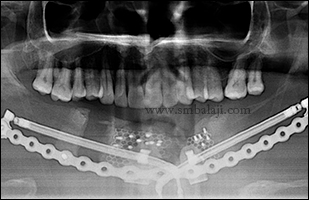
A young man from Singapore reported to me with the complaint of huge swelling in the right side of his face. He added that the size of the swelling was increasing progressively which made his face asymmetrical. He was very cautious about this progressive swelling. Added he had histopathological examination of the intraoral tissue done elsewhere diagnosing as plexiform ameloblastoma.
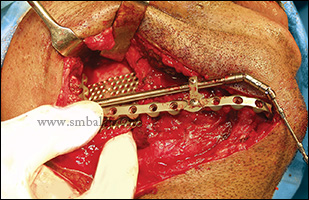
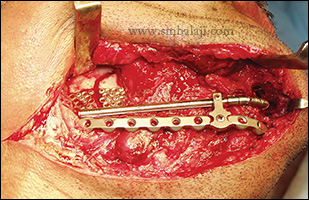
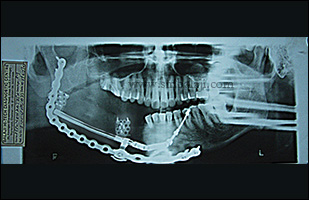
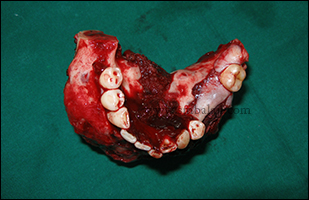
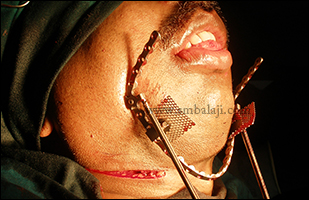
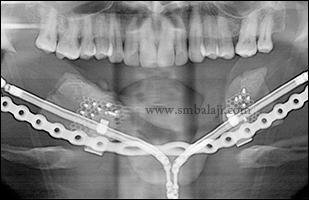
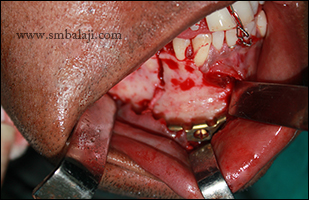
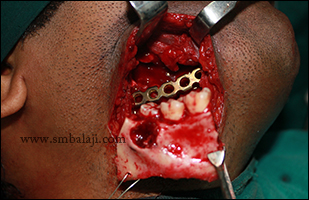
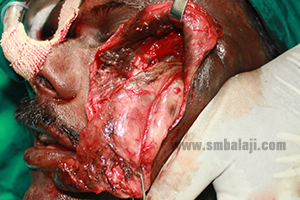
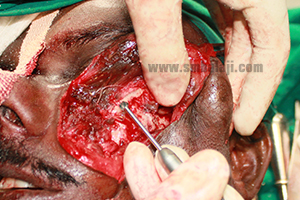
After thorough clinical and radiological examination, Maxillofacial Surgeon Dr. S. M. Balaji planned to remove the lesion and reconstruct the affected jaw portion in a single stage. Intraorally, complete removal of the benign lesion with sufficient clearance of the bone was done following rib graft which was obtained was fixed to it. Patient was happy to have both removal and reconstruction in a single surgery.
After thorough clinical and radiological examination, Maxillofacial Surgeon Dr. S. M. Balaji planned to remove the lesion and reconstruct the affected jaw portion in a single stage. Intraorally, complete removal of the benign lesion with sufficient clearance of the bone was done following rib graft which was obtained was fixed to it. Patient was happy to have both removal and reconstruction in a single surgery.







































 RSS Feed
RSS Feed