








A 5 year old boy was brought to our hospital with a complaint of decreased mouth opening and facial deformity by birth. His parent’s gave the history of multiple surgical correction of TMJ ankylosis done elsewhere. He had unsightly extraoral scar due to previous surgeries. He gave a history of having undergone distraction osteogenesis treatment for the left side of the lower jaw in some other hospital elsewhere, but the treatment subsequently failed.
Now on examination he had facial asymmetry, severely retruded lower jaw (mandible), flattened lower face with complete restriction in mouth opening and shift of chin towards left side.
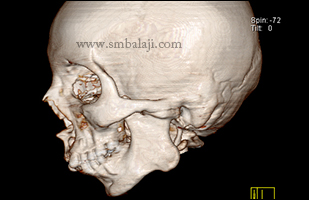
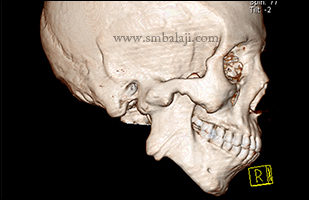
3DCT of facial bones revealed obliterated left temporomandibular (joint jaw) joint space, elongated coronoid process, and reduced ramal height and prominent antegonial notch. The case was diagnosed as true left TMJ bony ankylosis with developing secondary facial deformity.
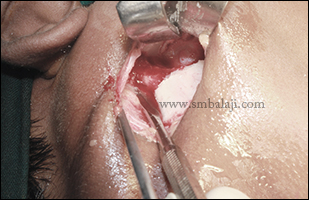
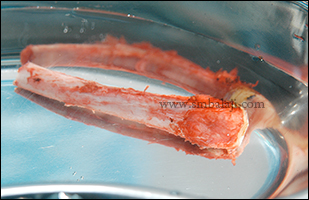
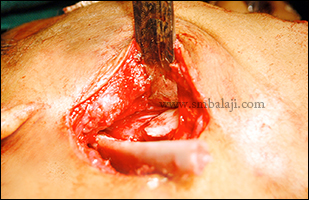
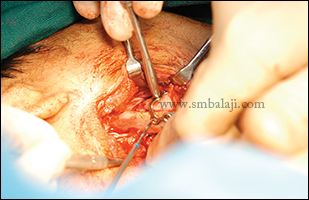
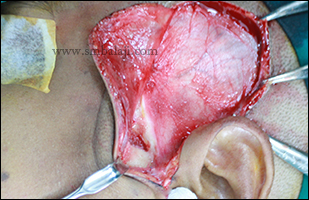
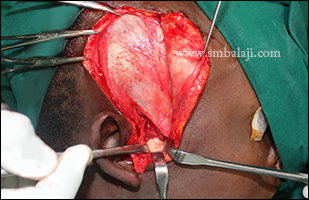
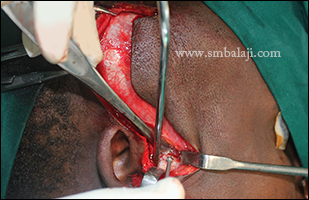
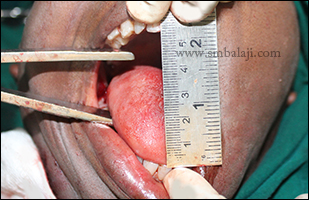
Maxillofacial Surgeon Dr. S. M. Balaji successfully performed bony ankylosis release surgery and transportation of growth centre using costochondral junction obtained from rib cartilage. Postoperative mouth opening was adequate. Following complete dental rehabilitation done to treat the badly broken and decayed teeth, boy’s parents were asked to continue the mouth opening exercise at least 2 months after surgery.
Now on examination he had facial asymmetry, severely retruded lower jaw (mandible), flattened lower face with complete restriction in mouth opening and shift of chin towards left side.
3DCT of facial bones revealed obliterated left temporomandibular (joint jaw) joint space, elongated coronoid process, and reduced ramal height and prominent antegonial notch. The case was diagnosed as true left TMJ bony ankylosis with developing secondary facial deformity.
Maxillofacial Surgeon Dr. S. M. Balaji successfully performed bony ankylosis release surgery and transportation of growth centre using costochondral junction obtained from rib cartilage. Postoperative mouth opening was adequate. Following complete dental rehabilitation done to treat the badly broken and decayed teeth, boy’s parents were asked to continue the mouth opening exercise at least 2 months after surgery.

























 RSS Feed
RSS Feed