
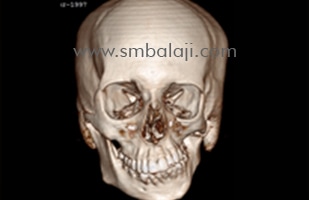
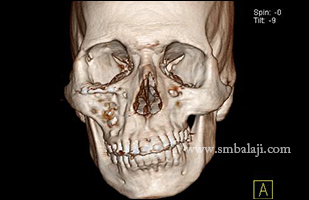
This lady has had long standing facial asymmetry with deviation of the mandible to the left side due to vertical shortening of the ramus on the left and an occlusal cant with resultant malocclusion. She presented to our hospital for correction of her deformity.
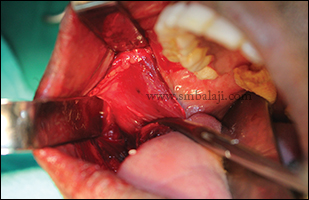
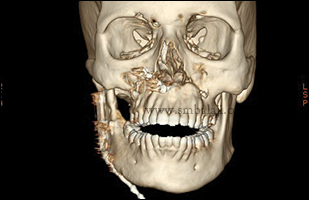
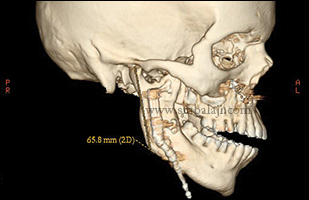
She underwent mandibular distractor placement along with a Le Fort I surgery. She subsequently underwent a mandibular distraction of 2 cm after a latency period of seven days. The distractor was removed after consolidation of bone at the distracted site in six months.
There was establishment of facial symmetry along with correction of the occlusal cant. She was very happy with the results of the surgery.
She underwent mandibular distractor placement along with a Le Fort I surgery. She subsequently underwent a mandibular distraction of 2 cm after a latency period of seven days. The distractor was removed after consolidation of bone at the distracted site in six months.
There was establishment of facial symmetry along with correction of the occlusal cant. She was very happy with the results of the surgery.






































 RSS Feed
RSS Feed