
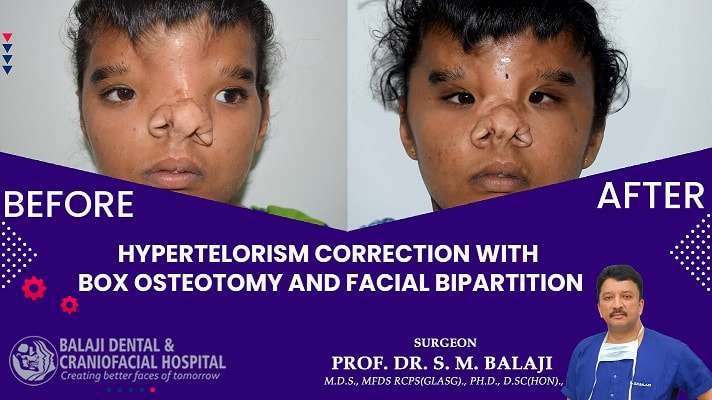
This young girl with hypertelorism was first operated on when she was six years old. Her parents presented with her once she had completed bone growth as instructed at the time of the initial surgery for further corrective surgery. A revision hypertelorism surgery was planned with a box osteotomy and facial bipartition procedure.
Comprehensive studies were obtained preoperatively including axial section CT scans of the facial bones. A mock surgery was then performed on a 3D stereolithographic model of her skull in consultation with the neurosurgical team that was closely involved in each step of the treatment process.
A bicoronal flap was raised and craniotomy was performed after removing previous screws and plates. Extreme care was taken to ensure that there was no damage to the duramater and the traditional frontal bar cut was performed.
Care was taken to preserve the olfactory bulb while handling the crista galli region. The segmental cuts were made with great care and medial nasal part was removed. This was followed by the orbital cut of the box osteotomy, which was performed as planned. Great care was exercised while handling the nasolacrimal duct to ensure that there would be no complications in the future.
The lower cut performed intraorally would result in movement of the midfacial segment alone and not the entire alveolus. After completely mobilizing the midfacial segments and removal of excess tissue, the edges were approximated. The frontal bar served as a standard guide for this procedure. They were secured with plates and screws. The position of external eye and nose were rechecked. Then the incisions were closed in layers.
There was optimal correction of the patient’s hypertelorism following the surgery. She would need a series of further surgeries to complete the rehabilitation process.
Comprehensive studies were obtained preoperatively including axial section CT scans of the facial bones. A mock surgery was then performed on a 3D stereolithographic model of her skull in consultation with the neurosurgical team that was closely involved in each step of the treatment process.
A bicoronal flap was raised and craniotomy was performed after removing previous screws and plates. Extreme care was taken to ensure that there was no damage to the duramater and the traditional frontal bar cut was performed.
Care was taken to preserve the olfactory bulb while handling the crista galli region. The segmental cuts were made with great care and medial nasal part was removed. This was followed by the orbital cut of the box osteotomy, which was performed as planned. Great care was exercised while handling the nasolacrimal duct to ensure that there would be no complications in the future.
The lower cut performed intraorally would result in movement of the midfacial segment alone and not the entire alveolus. After completely mobilizing the midfacial segments and removal of excess tissue, the edges were approximated. The frontal bar served as a standard guide for this procedure. They were secured with plates and screws. The position of external eye and nose were rechecked. Then the incisions were closed in layers.
There was optimal correction of the patient’s hypertelorism following the surgery. She would need a series of further surgeries to complete the rehabilitation process.
 RSS Feed
RSS Feed